
 Member
Member- Jul 31, 2014
- 284
- Tinnitus Since
- July 14, 2014
- Cause of Tinnitus
- Assault/Contusion/Ear Infection
Hi Dr. Nagler,
Have a question about my DPOAE test and if that is the cause of my T. My audiogram looks normal for my age. I'm in my mid 30's.
Background:
My T started 50 days after a physical assault to my ears and head which triggered High intracranial pressure and an ear infection. Note: I got a Lumbar Puncture to fix my ICP, my T lowered but did not go away.
My left ear is ringing more than the right ear.
1. Do you think the weak cochlear outer hair cell around 5700 Hz are due to the assault or something else?
2. Is the dip in my left ear around 5700 Hz causing my Tinnitus, if so why would my right ear ring?
3. Is my T more Neurological due to Head Injury.
Please see DPOAE chart.
My ENT thinks my T is more Neurological but I emailed my Audiologist and below is what he had to say.
Email from my Audiologist:
I suppose it is possible that the tinnitus is due to less robust cochlear outer hair cell function around 5700 Hz in your left ear , especially since the more recent tinnitus match you did came closer to that frequency than we originally though. However, like I said, the emissions are weaker but still present which means there is still outer hair cell function at that frequency. We may never know for sure one way or the other.
Another email from Audiologist before I measured my T to be around 6000 Hz:
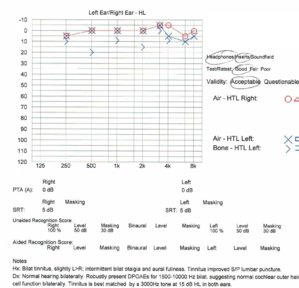
The DPOAE generated by your ear is represented by the circle markers for the right ear and the circle/X markers for the left ear. From that perspective, the amplitude response of your DPOAEs as a function of frequency in your right ear is about as flat as they come. In your left ear, you are correct that there is a dip in amplitude at around 5700 Hz. It is possible that this reflects less strong cochlear outer hair cell function around 5700 Hz than at the other test frequencies, especially given that you reported stronger tinnitus in the left, although perceptually your tinnitus corresponded closest to a 3000 Hz tone. However, this dip just as likely reflects a stimulus standing wave artifact, which is very common for frequencies around 6000 due to the length of the ear canal.
The triangle markers below each DPOAE marker represent the noise floor for the same frequency band in which that particular DPOAE is measured. We are most concerned with the DPOAE signal to noise ratio, represented by the distance between the DPOAE marker and the corresponding triangle below it. All of your responses, even at 5700 Hz in the left ear, are robust with high signal to noise ratios, indicating that the cochlear outer hair cells are functioning throughout the frequency range measured. So I am not concerned that there is some problem that the MRI did not pick and I do not believe you should be either.
Here is a previous thread about my T.
https://www.tinnitustalk.com/threads/tinnitus-spikes-when-i-bite-my-molars.7361/
Thanks so much!
Have a question about my DPOAE test and if that is the cause of my T. My audiogram looks normal for my age. I'm in my mid 30's.
Background:
My T started 50 days after a physical assault to my ears and head which triggered High intracranial pressure and an ear infection. Note: I got a Lumbar Puncture to fix my ICP, my T lowered but did not go away.
My left ear is ringing more than the right ear.
1. Do you think the weak cochlear outer hair cell around 5700 Hz are due to the assault or something else?
2. Is the dip in my left ear around 5700 Hz causing my Tinnitus, if so why would my right ear ring?
3. Is my T more Neurological due to Head Injury.
Please see DPOAE chart.
My ENT thinks my T is more Neurological but I emailed my Audiologist and below is what he had to say.
Email from my Audiologist:
I suppose it is possible that the tinnitus is due to less robust cochlear outer hair cell function around 5700 Hz in your left ear , especially since the more recent tinnitus match you did came closer to that frequency than we originally though. However, like I said, the emissions are weaker but still present which means there is still outer hair cell function at that frequency. We may never know for sure one way or the other.
Another email from Audiologist before I measured my T to be around 6000 Hz:
The DPOAE generated by your ear is represented by the circle markers for the right ear and the circle/X markers for the left ear. From that perspective, the amplitude response of your DPOAEs as a function of frequency in your right ear is about as flat as they come. In your left ear, you are correct that there is a dip in amplitude at around 5700 Hz. It is possible that this reflects less strong cochlear outer hair cell function around 5700 Hz than at the other test frequencies, especially given that you reported stronger tinnitus in the left, although perceptually your tinnitus corresponded closest to a 3000 Hz tone. However, this dip just as likely reflects a stimulus standing wave artifact, which is very common for frequencies around 6000 due to the length of the ear canal.
The triangle markers below each DPOAE marker represent the noise floor for the same frequency band in which that particular DPOAE is measured. We are most concerned with the DPOAE signal to noise ratio, represented by the distance between the DPOAE marker and the corresponding triangle below it. All of your responses, even at 5700 Hz in the left ear, are robust with high signal to noise ratios, indicating that the cochlear outer hair cells are functioning throughout the frequency range measured. So I am not concerned that there is some problem that the MRI did not pick and I do not believe you should be either.
Here is a previous thread about my T.
https://www.tinnitustalk.com/threads/tinnitus-spikes-when-i-bite-my-molars.7361/
Thanks so much!

 Member
Member