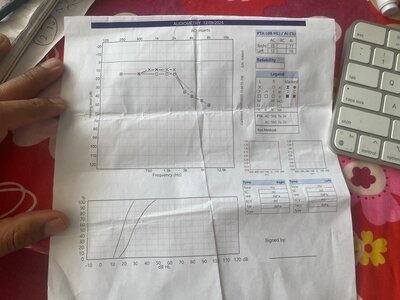
Your audiogram indicates hearing loss.
No question.
I would say a significant amount of hearing loss.
My next question would be, how old are you, and what kind of work or recreational activities resulted in this level of hearing loss?
An assumption about the true state of your hearing based on so few data points in your chart is tenuous. How much hearing loss you have, and which frequencies are mostly lost, cannot be determined from your chart.
Audiograms like this use whole 1000 Hz intervals and increments of around 5 dB. They are quick and basic.
Because only a few data points are taken, a lot of information is missing. Plotting the audiogram on a logarithmic scale, as is done here, can also be misleading when you want to understand the true nature of your hearing loss. This is a common problem with audiologist audiograms. The use of a log scale and minimal data points is a lazy convention followed by many audiologists.
Here is a study where the researchers considered 14 data points over 16,000 Hz to be an extended hearing test:
A PhD dissertation that concludes that GPIAS works in humans. Change in Acoustic Startle as an Indicator of Continuous Tonal Tinnitus Abstract: Currently, there is no accepted objective measure of tinnitus in humans. The gap prepulse inhibition of acoustic startle (GPIAS) paradigm is an...

www.tinnitustalk.com
Describing 14 data points over 16,000 Hz as an "extended audiogram" may be valid, but it still does not provide enough useful data.
I once described a sparse hearing test of 6 data points over 8000 Hz to an engineer friend over the phone. Without knowing anything about hearing, his immediate response was something he remembered from a statistics lecture: you would need at least 30 data points over that range, or about 4 per thousand hertz. Anything less, and you do not have enough data to make reliable conclusions.
It is not complicated to perform a more intensive audiogram yourself.
My chart includes embedded instructions so that you and I can both reproduce the process:
The way I look at it is that you have a "perfect audiogram" (almost). Clearly your hearing isn't perfect as you suffer from tinnitus. A perfect audiogram is a necessary condition to perfect hearing, but not sufficient. Audiograms have important limitations, many of which you can find mentioned...
www.tinnitustalk.com
I took about 40 evenly spaced measurements and later repeated the process after adjusting for high-frequency hearing loss.
It is unlikely that you will find a discrete tone that corresponds exactly to your white noise tinnitus. White noise means many frequencies are present at similar volumes.
You should also be aware that tones are not always whole numbers in hertz; you can have single-hertz increments, for example, 7344.50 Hz. Tonal tinnitus can drift. My own high-frequency tinnitus shifts within a range.
You should be able to describe your white noise tinnitus as higher or lower than a certain frequency threshold, for example, higher than 7200 Hz.
If you focus carefully, you may also detect some pure tones. In my case, I had one pure tone in my left ear. When I looked for it, I realized there was also another sound—white noise—lower in frequency but still high-pitched and not a pure tone.
The Audio Notched White Noise Therapy example I mentioned earlier assumes reasonable hearing on both sides of the tinnitus and hearing loss region, forming a curve similar to a sine wave. This is an assumption about the patient's hearing and tinnitus.
Is this assumption valid in your situation?
In my case, and likely in yours as well, the high-frequency white noise tinnitus occurs in the region where hearing has sharply deteriorated. Hearing loss and tinnitus usually go hand in hand in cases of auditory trauma.
At lower frequencies, you have relatively good hearing (as seen in your chart), while at higher frequencies, hearing has deteriorated (also visible in your chart). That line of deterioration continues in the higher frequency range, beyond what is currently measured. You can measure this further loss yourself.
If you play a notched therapy sound, whether pure tones or white noise, you will hear the lower-frequency therapy sounds (where hearing is reasonable), while the higher-frequency sounds will be inaudible due to your deteriorated hearing.
Your hearing does not follow the assumed bell-shaped curve that Notched Therapies describe.
The assumption that you have good hearing on both sides of your tinnitus tone is invalid.
You would need to increase the volume of the high-frequency range of your therapy sound—likely into a range that could cause further damage—while keeping the lower-frequency range moderate or low to avoid harming the parts of your hearing that are still functional.
I am not sure that Notched Therapy sounds are sophisticated enough to adjust the volume in this way, or if they are, how users can fine-tune them to match their needs.
It seems that Notched Sound Therapy relies on the idea that the auditory system tries to recruit nearby hearing cells close to the frequencies where hearing loss and tinnitus occur, even if it does not explicitly state this.
Below is a paragraph from the following link:
"A dedicated section on notched sound therapy explores its mechanism of action, which leverages the principle of lateral inhibition to suppress the hyperactive auditory neurons responsible for the phantom sound. Clinical studies, including a seminal 2009 PNAS study and a recent 2025 meta-analysis, provide evidence that this therapy can significantly reduce tinnitus loudness and emotional distress, particularly for patients with tonal tinnitus."
Executive Summary Tinnitus is a prevalent and often debilitating condition characterized by the perception of internal sound in the absence of an external source. It affects millions of individuals…

soundofmind.app
The term "lateral inhibition" refers to how hearing cells adjacent to the tinnitus and hearing loss frequencies are recruited to respond to nearby tones. If successful, they can again send signals to the brain corresponding to those frequencies, allowing the brain to suppress or resolve the tinnitus it is generating.
Notched Audio Therapies deliver targeted sounds on either side of the tinnitus and hearing loss frequencies to enhance this recruitment process.
The hearing cell recruitment model is well-known in tinnitus research and is active in most patients.
For those with early-stage tinnitus and relatively good hearing near the affected frequency range, hearing cell recruitment can be effective in reducing or resolving tinnitus.
People often attribute their recovery to a specific treatment or belief, when in reality, their auditory system's recruitment process reduced or eliminated the tinnitus on its own.
Your hearing loss does not follow a bell-shaped curve as Notched Sound Therapies assume.
You might identify such a pattern if you conduct a more detailed hearing test. You may also discover a pure tone tinnitus or describe your white noise as higher or lower than a certain threshold.
You can only perform this test yourself. No practitioner will spend the necessary time and effort.
If your tinnitus pitch varies, you may need to wait until hearing cells deteriorate further and your brain consolidates multiple tones into one or a general white noise region.
Alternatively, your auditory system may find another compensatory pathway. However, I suspect that hearing cell recruitment may no longer play a role in your case, because your chart does not show any curve resembling a sine wave.
In my own detailed audiogram, both ears showed a curve at about 4250 Hz, but that is not where my tinnitus is.
Hearing cell recruitment is an ongoing, lifelong process that occurs as hearing naturally declines. It does not simply begin when tinnitus or major hearing loss first appears.